
What is sleep-disordered breathing in children?
Sleep-disordered breathing (SDB) in children encompasses a spectrum of conditions ranging from primary snoring to obstructive sleep apnea, affecting between 2% and 5% of children. These disorders, often underdiagnosed, can affect growth, cognitive development and behavior. The orthodontist plays a key role in their screening through examination of the maxillofacial structure.
The SDB spectrum includes, in increasing order of severity:
- Primary snoring : Vibration of soft tissues without breathing interruption. Affects 10 to 12% of children according to the American Academy of Pediatrics.
- Upper airway resistance syndrome (UARS) : Increased breathing effort leading to frequent micro-arousals and fragmented sleep.
- Obstructive sleep apnea (OSA) : Repeated breathing pauses with drops in blood oxygen levels. Occurs most frequently between ages 2 and 8.
Unlike adults, where daytime drowsiness dominates, children with SDB often present with hyperactivity, irritability and difficulty concentrating, which complicates diagnosis.

How to recognize sleep disorders in your child?
Sleep-disordered breathing shows through nighttime and daytime signs. If your child presents several of these symptoms, consult a professional.
🌙 Nighttime signs
- Regular snoring (more than 3 nights per week)
- Breathing pauses observed by parents
- Mouth breathing during sleep
- Neck hyperextension (head tilted backward)
- Excessive sweating at night
- Restless sleep, unusual positions
- Bruxism (teeth grinding)
- Persistent bedwetting
- Frequent nightmares or night terrors
☀️ Daytime signs
- Excessive fatigue and drowsiness
- Difficulty concentrating and declining school performance
- Hyperactivity and impulsive behavior
- Irritability, mood swings
- Morning headaches
- Pronounced dark circles under the eyes
- Open mouth at rest
- Permanent mouth breathing
👁️ Physical and orthodontic signs
- Narrow and deep palate (V-shaped palatal vault)
- Long and narrow face (adenoid facies)
- Receding chin (mandibular retrognathism)
- Anterior open bite (upper and lower teeth don't touch)
- Visibly enlarged tonsils
- Low tongue position at rest
Checklist for parents, Does your child show these signs?
If you check 3 items or more, an airway evaluation is recommended.
Why do some children develop sleep disorders?
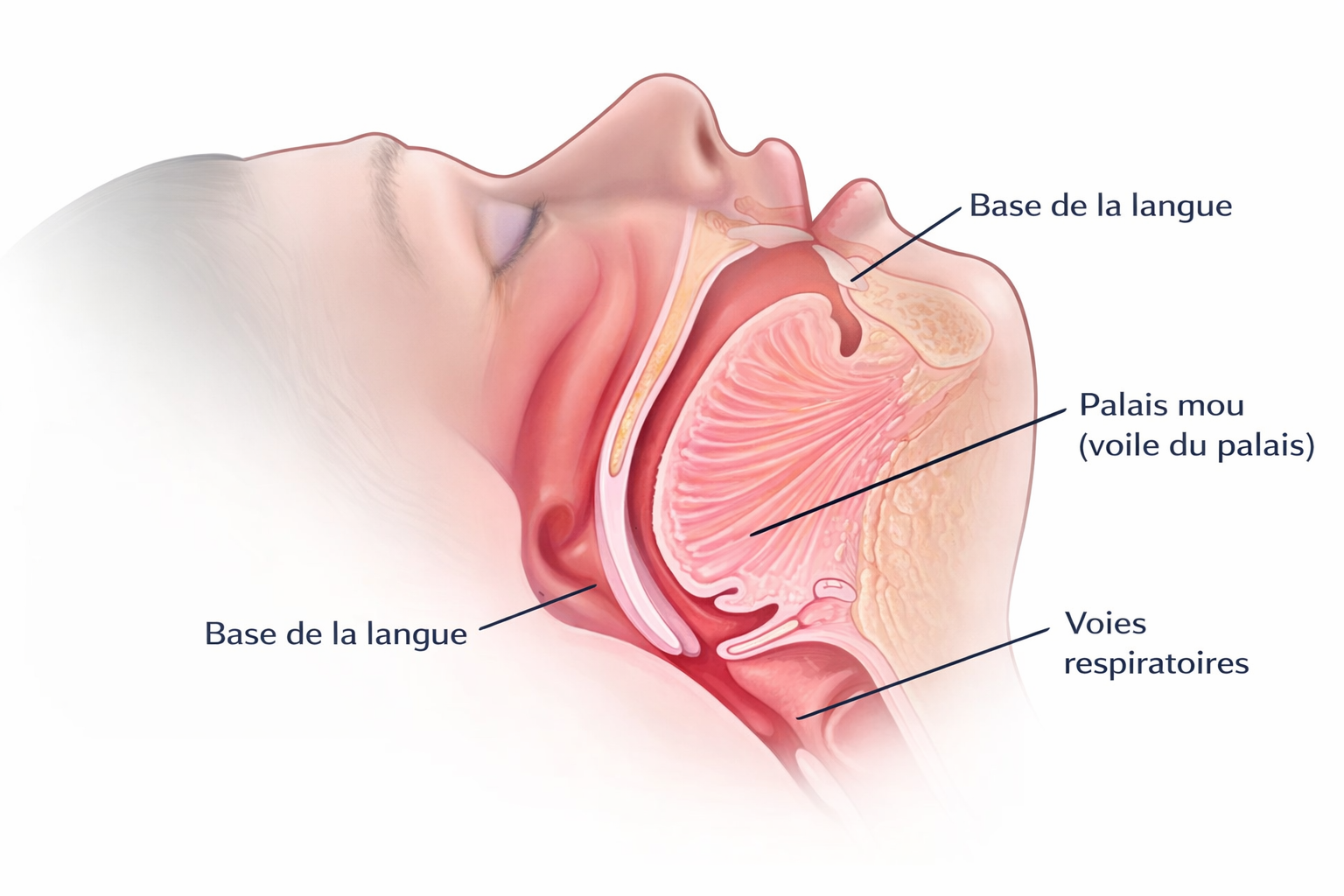
Sleep-disordered breathing in children mainly results from a physical obstruction of the upper airways, often related to craniofacial growth and lymphoid tissue hypertrophy.
Enlarged tonsils and adenoids
The most common cause in children. Large tonsils and adenoids physically reduce the air passage, especially when lying down. This problem peaks between ages 2 and 8.
Narrow palate and craniofacial anomalies
About 70% of children with sleep apnea have narrow maxillary structures. A V-shaped palate reduces nasal cavity volume and forces mouth breathing, creating a vicious cycle that worsens malocclusion.
Chronic mouth breathing
Mouth breathing alters facial development: the face elongates, the chin recedes, the tongue adopts a low position. This remodeling further reduces the airways, worsening SDB. Nearly 97.5% of mouth breathers have pronounced dark circles.
Aggravating factors
Obesity, chronic allergies (rhinitis, asthma), family history of sleep apnea and prematurity significantly increase the risk of SDB in children.
The key role of the orthodontist in screening
The orthodontist is often the first healthcare professional to detect signs of sleep-disordered breathing in children, as they regularly examine the jaw, palate, tongue position and bite, all indicators of airway patency.
During each consultation, Dr Benguira systematically evaluates:
- Palate width : A narrow palate is directly linked to reduced nasal volume and mouth breathing
- Mandibular position : A receding mandible (retrognathism) reduces posterior airway space
- Tonsil volume : Hypertrophy visible on oral examination
- Breathing habits : Nasal vs mouth breathing, tongue position at rest
- Screening questionnaire : Use of the scientifically validated Pediatric Sleep Questionnaire (PSQ)
The American Association of Orthodontists (AAO) recommends a first evaluation at age 7. Dr Benguira, with 15 years of experience at Sainte-Justine Hospital with complex patients, has particular expertise in pediatric airway evaluation.
Orthodontic treatments for sleep disorders
Orthodontics does not cure sleep apnea on its own, but it plays a major role in a multidisciplinary approach by widening the airways and correcting anatomical factors contributing to obstruction.
Rapid palatal expansion (RPE)
RPE widens the upper jaw by opening the mid-palatal suture, increasing nasal cavity volume. Ideal age: 7 to 14 years (suture still open). Studies demonstrate a 51.6% reduction in adenoid volume and a 75.4% reduction in tonsillar volume after expansion.
Mandibular advancement
Mandibular advancement appliances reposition the lower jaw forward, opening the posterior airways. Particularly effective in children with mandibular retrognathism (receding chin).
Interceptive orthodontics
Early treatment (Phase 1) guides jaw growth during the active development period. Orthodontic intervention can considerably reduce airway obstruction, decrease snoring and sometimes avoid surgery.
Myofunctional re-education
Orofacial re-education (myofunctional therapy) complements orthodontic treatment by reprogramming the facial muscles. The exercises aim to:
- Reposition the tongue : The tongue should rest against the palate, promoting nasal breathing
- Strengthen the lip muscles : Enabling lip closure at rest and during sleep
- Correct swallowing : Eliminating infantile swallowing that perpetuates the open bite and low tongue position
Diagnosis: polysomnography
The polysomnography (PSG) is the gold standard test for diagnosing sleep-disordered breathing. Performed in a sleep laboratory, it records:
- Oxygen saturation : Detection of desaturations related to apneas
- Heart rate : Cardiovascular effects of respiratory events
- Respiratory flow : Identification of apneas, hypopneas and micro-arousals
Home nocturnal oximetry offers a simplified alternative for initial screening.
Simple snoring vs Sleep apnea in children
Not all snorers have sleep apnea, but all snoring deserves attention. Here is how to tell the difference:
| Criteria | Primary snoring | Obstructive sleep apnea |
|---|---|---|
| Breathing | Continuous, without interruption | Repeated breathing pauses (apneas) |
| Blood oxygen | Normal | Repeated drops (desaturations) |
| Sleep | Generally restorative | Fragmented, non-restorative |
| Daytime behavior | Usually normal | Hyperactivity, irritability, fatigue |
| Growth | Not affected | Risk of growth delay |
| Prevalence | 10-12 % des enfants | 2-5 % des enfants |
| Diagnosis | Clinical | Polysomnography (gold standard test) |
The multidisciplinary approach
The optimal treatment of sleep-disordered breathing in children requires close collaboration between several healthcare professionals. The orthodontist often coordinates this approach with the ENT, pediatrician and sleep specialist.
Typical care pathway
- Step 1, Screening The orthodontist identifies clinical signs during the exam. The PSQ (Pediatric Sleep Questionnaire) is administered to parents.
- Step 2, Diagnosis Referral to the ENT and/or sleep specialist for polysomnography and complete evaluation.
- Step 3, Treatment plan Development of a joint plan: orthodontics (expansion, advancement), ENT surgery (adenotonsillectomy if indicated), re-education.
- Step 4, Active treatment Installation of orthodontic appliances and regular follow-up. Typical duration: 6 to 18 months.
- Step 5, Follow-up Evaluation of results on sleep, breathing and growth. Control polysomnography if necessary.
When is surgery necessary?
The adenotonsillectomy (removal of tonsils and adenoids) remains the first-line treatment for moderate to severe pediatric OSA. However:
- Palatal expansion alone may be sufficient in mild to moderate cases with narrow palate
- The combined approach (surgery + orthodontics) offers the best results in severe cases
- Interceptive orthodontics can reduce the need for later surgery
Dr Benguira works closely with ENTs in the region to provide complete care for every child.
When to consult an orthodontist for your child's sleep disorders?
Consult an orthodontist if your child shows signs of sleep-disordered breathing, ideally from age 6-7. Intervention during the active growth period offers the best chances of correcting anatomical abnormalities without surgery.
Consult urgently if:
- Observed breathing pauses : You notice your child stops breathing during sleep
- Intense daily snoring : Snoring audible from another room
- Unexplained school difficulties : Sudden drop in grades, behavior labeled as ADHD
- Growth delay : Growth hormone is primarily secreted during deep sleep
At Mon Orthodontiste, the orthodontic consultation is free. Dr Benguira performs a complete evaluation including airway examination, maxillofacial structure and a sleep screening questionnaire.

The consequences of untreated sleep disorders
Left untreated, sleep-disordered breathing in children can have serious and lasting effects on physical, cognitive and behavioral development.
Growth delay
Growth hormone (GH) is primarily secreted during deep sleep. Chronic SDB disrupts this secretion and can lead to growth retardation.
Academic and behavioral difficulties
Loss of concentration, impaired memory, hyperactivity, irritability, aggression. Many children receive an ADHD diagnosis when their real problem is a sleep disorder.
Abnormal craniofacial development
Chronic mouth breathing alters facial growth: elongated face, narrow palate, receding chin. These changes become permanent if not corrected during childhood.
Long-term complications
Cardiovascular problems (hypertension, irregular heart rhythm), persistent bedwetting, permanent malocclusion requiring more complex orthodontic treatment in adulthood.
Frequently asked questions about sleep disorders in children
Occasional snoring during a cold can be normal. However, regular loud snoring (more than 3 nights per week) is one of the main signs of sleep-disordered breathing. According to the American Academy of Pediatrics, habitual snoring affects 10 to 12% of children and warrants a medical evaluation.
The orthodontist regularly examines the jaw, palate and airway structure. A palate that is too narrow or a receding mandible reduces the air passage and promotes sleep-disordered breathing. Treatments like rapid palatal expansion can widen the airways and significantly improve your child's sleep quality.
The American Association of Orthodontists recommends a first evaluation at age 7. However, if your child shows signs of breathing disorders (snoring, mouth breathing, daytime fatigue) before that age, an early consultation is recommended. Intervention during the active growth period maximizes treatment effectiveness.
Rapid palatal expansion (RPE) is an orthodontic treatment that gradually widens the upper jaw by opening the mid-palatal suture. This expansion increases nasal cavity volume, improves air passage and promotes nasal breathing. Studies published in PubMed show a 51.6% reduction in adenoid volume and a 75.4% reduction in tonsillar volume after expansion.
Signs of mouth breathing include: parted lips at rest, dry mouth upon waking, pronounced dark circles under the eyes, snoring, long and narrow face, receding chin. Nearly 97.5% of mouth-breathing children have pronounced dark circles. A simple test: during sleep, place a small mirror under the nose, if there's no fog, your child is breathing through the mouth.
Yes, significantly. The lack of restorative sleep leads to concentration difficulties, memory problems, irritability and decreased academic motivation. Studies show that 25 to 50% of children diagnosed with ADHD have concurrent sleep disorders, suggesting that some ADHD diagnoses may mask a nighttime breathing problem.
Orthodontics does not cure sleep apnea on its own, but it plays a major role in a multidisciplinary approach. Rapid palatal expansion can significantly reduce the severity of apnea by widening the airways. The optimal treatment often combines orthodontics, ENT (surgery if necessary), myofunctional re-education and pediatric follow-up.
Left untreated, SDB can lead to: growth delay (growth hormone is secreted during deep sleep), academic difficulties, behavioral problems, permanent abnormal craniofacial development (adenoid facies), cardiovascular complications, persistent bedwetting and permanent malocclusion requiring more complex treatment in adulthood.
The link is well documented scientifically. Between 25 and 50% of children diagnosed with ADHD have concurrent sleep disorders. Sleep deprivation in children manifests as hyperactivity and inattention, mimicking ADHD symptoms. Dr Benguira, with 15 years of experience at Sainte-Justine with special needs children, systematically evaluates the airways of these patients.
Primary snoring is a vibration of soft tissues without breathing interruption or oxygen drop, while obstructive sleep apnea involves repeated breathing pauses with oxygen desaturation. Apnea can lead to cardiovascular, neurocognitive and growth consequences. Polysomnography is the gold standard test to differentiate between them.
Is your child sleeping poorly?
The orthodontic consultation is free and includes a complete airway evaluation. Early screening, adapted treatment, lasting results.
* Free consultation for orthodontics. Fees apply for TMJ, sleep apnea and neuromodulator consultations.
Articles on sleep and orthodontics
Sleep apnea and orthodontics
Discover our articles on the link between sleep disorders and orthodontics on our blog.
Read articles →Orthodontics for children
First consultation from age 7, interceptive and preventive treatment to guide your child's growth.
Learn more →Adult sleep apnea
Sleep apnea treatment with a dental appliance. CPAP alternative for adults.
Learn more →Dr David Benguira
Board-certified orthodontist FRCD(C) with over 20 years of experience, Dr Benguira practiced for 15 years at Sainte-Justine Hospital treating children with complex conditions, including sleep-disordered breathing, ADHD, autism and Down syndrome.
This unique experience gives him particular expertise in pediatric airway assessment and orthodontic treatment of sleep disorders in children.
Article reviewed on March 20, 2026 by Dr David Benguira, Orthodontist FRCD(C).
